How Much Does it Cost to Train a Physician in Colombia?
¿Cuánto cuesta formar a un médico en Colombia?
Quanto custa formar a um médico na Colômbia?
How Much Does it Cost to Train a Physician in Colombia?
Revista Ciencias de la Salud, vol. 16, no. 2, 2018
Universidad del Rosario
Received: 12 September 2017
Accepted: 09 March 2018
Additional information
To cite this article: Gil-Rojas Y, Gil-Tamayo S, Mosos JD, Hernández F,
Castañeda-Cardona C, Lasalvia P et al. How
Much Does it Cost to Train a Physician in Colombia? Rev Cienc
Salud. 2018;16(2):219-236. Doi: https://doi.org/10.12804/revistas.urosario.edu.co/revsalud/a.6767
Abstract: Introduction: The aim of this project is to estimate the costs to society of training a doctor at either a public or a private university in Colombia. Materials and methods: Direct and indirect costs were estimated in 2016 Colombian pesos (average exchange rate 3051 COP per US dollar), as was the return on investment, expressed as net present value, return on investment, and internal rate of return. The time required to recover the investment in studying medicine was also determined, and this was contrasted with the counterfactual of studying in another academic program. A discount rate of 12 % was used. A sensitivity analysis was performed with several alternative scenarios. Results: In the baseline scenario, the total cost of training a physician in Colombia is US $80, 971.80 at a private university and US $54, 971.79 at a public university (of which $14, 436.57 is contributed by the State in the latter case). The time to return of investment is 3 years 6 months for study at a public university and 7 years 3 months for study at a public university. Applying discount rates of 5 %, 7.5 %, and 12 %, studying medicine presents a higher return than that obtained by studying in another academic program. Conclusions: The cost of training a medical doctor in Colombia is 70 % higher than the cost of training other professionals, but returns are greater due to subsequent higher income. Net returns are higher for graduates of public universities because their initial investment is smaller and their incomes are similar.
Keywords: costs and cost analysis, medical education, undergraduate, medical schools, investments.
Resumen: Introducción: este estudio busca estimar los costos de formar un médico en Colombia, tanto en una universidad pública como privada, desde la perspectiva de la sociedad. Materiales y métodos: se calcularon los costos directos e indirectos en pesos colombianos de 2016 (tasa de cambio promedio 3051 COP por USD), así como el retorno a la inversión, expresado en valor actual neto, retorno sobre la inversión, y tasa interna de retorno y, el periodo de recuperación de la inversión de estudiar medicina frente al contrafactual de estudiar otra carrera. Se empleó una tasa de descuento de 12 %. Se realizó un análisis de sensibilidad con varios escenarios. Resultados: en el escenario base, el costo total de la formación de un médico en Colombia es de $80 971.80 USD en una universidad privada y de $54 971.79 USD en una pública (de los cuales $14 436.57 USD son aportados por el Estado). El tiempo de retorno de la inversión es de 3 años y 6 meses en una universidad pública y 7 años y 3 meses en una privada. Aplicando tasas de descuento de 5 %, 7,5 % y 12 %, estudiar medicina presenta mayor retorno que el obtenido con otra carrera. Conclusiones: el costo de formación de un médico en Colombia es un 70 % mayor al requerido para la formación de otro profesional; sin embargo, los retornos son mayores debido los mayores ingresos percibidos. Los retornos son mayores en los egresados de universidades públicas, debido a que la inversión es menor y los ingresos percibidos son similares.
Palabras clave: costos y análisis de costo, educación de pregrado (licenciatura) en Medicina, facultades de Medicina, inversiones en salud.
Resumo: Introdução: o objetivo deste trabalho é estimar os custos de formar um médico na Colômbia, tanto em uma universidade pública quanto privada, desde a perspectiva da sociedade. Materiais e métodos: calcularam-se os custos diretos e indiretos em pesos colombianos de 2016 (taxa de câmbio médio 3051 COP por USD) assim como o retorno ao investimento, expressado em valor atual neto, retorno sobre o investimento, e taxa interna de retorno e, o período de recuperação do investimento de estudar medicina frente ao contrafactual de estudar outra carreira. Empregou-se uma taxa de desconto de 12 %. Se realizou uma análise de sensibilidade com vários cenários. Resultados: no cenário base, o custo total da formação de um médico na Colômbia é de $80 971.80 USD em uma universidade privada e $54 971.79 USD em uma pública (dos quais $14 436.57 USD são aportados pelo Estado). O tempo de retorno do investimento é de 3 anos e 6 meses em uma universidade pública e 7 anos e 3 meses em uma privada. Aplicando taxas de desconto de 5 %, 7.5 % e 12 %, estudar medicina apresenta maior retorno que o obtido com outro curso. Conclusões: o custo de formação de um médico na Colômbia é um 70 % maior ao requerido para a formação de outro profissional, no entanto, os retornos são maiores devido aos maiores ingressos percebidos. Os retornos são maiores nos formados de universidades públicas, devido a que o investimento é menor e os ingressos percebidos são similares.
Palavras-chave: custos e análise de custo, educação de graduação (licenciatura) em Medicina, faculdades de Medicina, investimentos em saúde.
Introduction
The cost of educating a medical student in monetary terms, in time, and in effort is one of the factors that determines the number of candidates who apply to medical programs. This cost should be related in some way to the return on investment (1). Due to concerns that the costs of educating medical students could limit access to the profession, an interest in calculating the cost of undergraduate medical education at United States universities arose at the end of the last century educational costs (instructional costs plus the costs of general supervision (2, 3, 4, 5). It was also thought that the availability of this data would be useful to request State financing.
Training a physician is a complex process, the economic costs of which are not limited to university tuition (2, 3, 4, 5). They also include the use of educational loans with the accrual of interest and a variety of other costs associated with food, housing, transportation, and materials (1, 2, 3, 4, 5, 6). Another factor is the loss of income that secondary school graduates could otherwise be earning while they are studying medicine.
In order to enter undergraduate university programs in Colombia, students must present secondary school diplomas and document their results on a State exam given to graduating high school students by the Colombian Institute for the Promotion of Higher Education (Instituto Colombiano para el Fomento de la Educación Superior – ICFES). Individual universities also have their own admission requirements, which in some cases include entrance exams. The National System for Information on Higher Education (Sistema Nacional de Información de la Educación Superior – SNIES) reported that in 2016 there were 55 medical programs in the country. Eighteen of them were public and 37 were private, all of them lasting 12-14 semesters. They granted diplomas in medicine, general medicine, or surgery, any one of which authorized their graduates to practice medicine. Out of the 41, 163 students in these programs, 74 % were studying at private universities. An average 261 credits were required for graduation from the public universities, and an average 274 credits were required for graduation from private universities (7).
The number of people applying to undergraduate medical programs in Colombia is much greater than the number of people who are admitted. In addition, medical programs are not available throughout much of the country, so there is significant migration of students from their municipalities of origin to the cities where these academic programs are available. In many cases, this increases the cost of education to students’ families or guardians. The MEDEA Study published in 2001, whose goal was to estimate the availability of doctors in 12 medical specialties in Colombia, indicated that the number of specialists has increased in recent years and will continue to increase, but that one of the primary problems was that the opening of new programs in medical specialties has not been based on the country’s needs. This has led to a deficit of physicians in certain specialties and has promoted a concentration of specialists in certain regions, which can make it difficult for graduates of specialized programs to find appropriate work placements (8). An additional problem is a growing number of general practitioners who seek positions in different specialties, although the demand for specialists in these fields has not been clearly studied (9). At the same time, the high cost of tuition charged to residents in certain fields is a disincentive for students with limited resources, who are otherwise most likely to choose to work in areas with unmet needs (8). While the cost of higher education in the country has been studied, no research focusing specifically on the cost of medical education is presently available. In light of the above, this research project seeks to estimate the social cost of training a physician in Colombia.
Materials and methods
A descriptive study and an economic model to estimate the social costs of training a physician in Colombia were developed. Because the perspective is the cost to Colombian society, both direct and indirect costs were considered.
The costs of physician training in the public and private sectors were calculated separately. In both cases, all accredited medical programs were included in the study. Data were obtained through official channels of each university and projections were made based principally on reviewing local databases and surveying a group of students regarding aspects for which no information was available. The resulting costs were expressed in dollars at constant prices for the year 2016. The information was processed in Excel®, and an average cost estimate was made for both public and private universities. An additional estimate was made reflecting weighted costs based on the number of students in each program.
Direct Costs
Direct costs are the expenditures necessary for access to higher education, including tuition, fees, other expenses, and costs covered by the community.
Tuition and Fees
The tuition and fees billed by universities represent the expenses incurred by students and/or their families to cover registration, tuition, and graduation and other fees. Tuition information was obtained from SNIES when it was available. When this information was not available from SNIES, it was sought from official sources at each university. In the case of public universities, tuition is calculated individually for each student, based on formulas established at the discretion of each institution. These formulas are applied to the socioeconomic profile of the student and his or her family (10). Data used was based on the following parameters: a stratum 3 student 4TN who was economically dependent, who lived with his or her parents, who had no children or any other dependents, who had graduated from a public secondary school or from a private secondary school whose tuition was average in relation to the range of tuitions considered by the university in question, and who lived in a household whose income was equivalent to the average household income reported by the National Administrative Department of Statistics (Departamento Administrativo Nacional de Estadísticas – (DANE) in 2007 for the capital city of the department where he or she was studying, as measured by its percentage of the Minimum Monthly Salary (Salario Mínimo Mensual Legal Vigente – SMMLV) in 2016 (table 1).
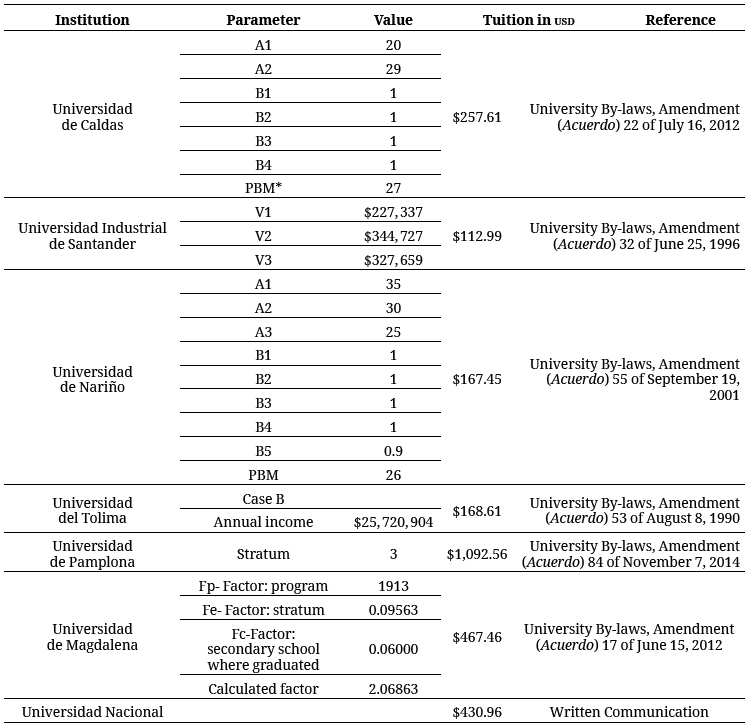
The web sites of the different universities were consulted to determine application and graduation fees. Application fees are paid by all applicants to a particular program and cover the cost of admissions processing (specific tests, interviews, etc.). Graduation fees cover the cost of the physical production of diplomas and in some cases the cost of the graduation ceremony. Application and graduation fees were calculated just once for each program, while tuition fees were estimated for each academic year until the program was completed.
Because both tuition fees and the number of students vary for each medical program, the calculation of tuition, application, and graduation fees was weighted based on the number of students enrolled in each program. When calculating the total cost of programs, their duration was taken into consideration, and used to determine the tuition charged to each student based on the socioeconomic profile of the student and his or her family. The duration of these programs ranged from 12-14 semesters.
Other Expenses
Other expenses incurred by families and or students who are associated with university studies were also considered. These costs included transportation, housing, food, books, photocopies, and other materials, including medical instruments. An electronic survey of medical students at different public and private universities in the country was used to estimate these costs, with the exception of the cost of medical instruments. Specifically, the survey was used to estimate the expenditures of students for food, housing, transportation, books, notebooks, photocopies, and biosafety equipment, including lab coats, gloves, face masks, and headwear. For convenience, this information was obtained from students who chose to participate voluntarily. In the case of medical instruments, it was assumed that at some point in their studies, all medical students would obtain a sphygmomanometer, a stethoscope, and an oto-ophthalmoscope. Basic and functional models of these instruments were priced based on availability, recognition, and recommendations. Their availability through the Pan-American Health Organization and in Colombia through the Ministry of Health and Social Protection was also taken into consideration.
Costs to the Community
This refers to State contributions to public education. Since the State provides a significant proportion of the resources needed to educate students at public universities, State budget allocations to each university were determined based on statistical reports issued by the universities and published in SNIES for the years 2003 and 2012 (7). Since no information was available regarding the allocation of resources to each program, it was assumed that the State’s per-student contribution to all programs was equal.
Indirect Costs
Among other indirect costs, lost income (lucrum cessans) due to students’ late entry into the labor market was also taken into consideration. In order to estimate lost income, i.e. the amount of money that a student could generate if he or she performed remunerated work during the years of his or her undergraduate studies, research was conducted on the average earnings of recent secondary school graduates, using data available through the Ministry of Education’s Observatory on Labor and Education (Observatorio Laboral para la Educación). The amount that students could earn per semester during the average six-year duration of a medical program was calculated. Based on the 2012 and 2013 minimum monthly salary, calculating income earned as measured against the minimum monthly salary by recent secondary school graduates (11.4 %) and applying this data to the minimum monthly salaries for the period of 2011-2016, the average monthly salary of a secondary school graduate was expressed in 2016 values (11). This analysis assumes that the opportunity cost of studying medicine would be to enter the labor market and earn as much as the average secondary school graduate.
Estimate of Total Costs
The average total cost of studying medicine was estimated by adding the direct and indirect costs. Total costs were estimated separately for public and private universities.
Benefits of the Investment
In order to provide the model with a comparator, the economic returns of studying medicine versus studying in any other university program were compared. The tuition costs for studying in other programs were obtained from the statistical report on higher education published by the Education Ministry, taking into account only those institutions at the university level. Because the values reported by the Ministry corresponded to the year 2015, they were updated to 2016 by applying the rate of inflation as reported in the Consumer Price Index. Other education costs (application and graduation fees) were assumed to be the same as for medical students (12). While there may be differences in expenditures related to the materials required during the program, the same values in this area were applied in the case of the counterfactual program other than medicine. This was based on the idea that while there may be programs requiring costly instruments, there may also be others where the cost of instruments is minimal.
Indirect costs were estimated by recalculating lost income, because the average duration of programs other than medicine is five years.
Various methods were applied to evaluate the benefits of the investment: net present value (NPV), return on investment (ROI), internal rate of return (IRR) and the investment recovery period. NPV corresponds to the difference between the current value of benefits in the form of income, and the current value of investments (13). The IRR is the discount rate at which NPV is equal to zero, i.e. the current value of benefits is equal to the current value of the investment (13). The cost/benefit or desirabilty ratio is obtained by dividing the discounted benefits at year zero by the discounted costs at year zero (13). The time for return on investment, known as tri, payback period, or recovery period, determines the amount of time it will take to recover an investment, i.e. the time required for net cash inflows to equal the initial investment (13). For the NPV, ROI, and tri, the period of evaluation is considered to be the 40 years subsequent to the investment. The selection of this time frame is based on research regarding returns from education (14).
In evaluating the returns from studying medicine or another university program, a scenario was constructed that considered only the income of graduates and applied a discount rate of 12 %, the rate recommended for public investment projects by the National Planning Department (Departamento Nacional de Planeación – DNP). Increments to the minimum salary were not considered in this analysis because earnings are constant. Income information was obtained from the Labor Observatory of the Ministry of Education in its data cube on the employment situation (15).
The information provided by different universities was consulted and the number of graduates as well as their income was recorded during the period in order to obtain a weighted average of the income of graduates of both public and private universities (16). Information from all 18 public universities was obtained, but 5 of the 37 private universities were excluded since they did not have the required information on the number of graduates or their income. The income data that was obtained was subsequently calculated to be expressed as a multiple of the minimum salary. Income in subsequent years was projected using this information. To obtain their medical degrees after completing their studies, students must carry out Obligatory Social Service (Servicio Social Obligatorio – SSO), previously known as their “rural year” (año rural). Thus, it was assumed that in the first year after completing their studies, their income and expenses where those that corresponded to the SSO. Because Resolution 2358 of 2014 authorized the Ministry of Health to assign these obligatory positions, it was possible to obtain salary information as published in the Ministry’s bulletin listing available placements as of July 19, 2016 (17, 18). It is assumed that monthly income was the average remuneration established on the list of available positions. Seventy percent of the positions listed no incentive other than the indicated remuneration, so it is assumed that most participants paid for their own subsistence during the year. In the case of graduates from programs other than medicine, average incomes were derived from figures published by the Labor Observatory of the Ministry of Education, excluding data pertaining to medical graduates (15).
Sensitivity Analysis
Various scenarios were projected for evaluating the economic benefits of medical studies. In these models, we considered different discount rates, increased income resulting from annual increases of the minimum salary, income variation based on the inclusion of expenses, and an analysis of economic benefits if educational loans are taken into consideration. Discount rates of 5 % and 7.5 % were considered. An annual increase of 5 % in the minimum salary was considered, since that was the average annual increase over the last five years (11). Information on spending was obtained from the Dane’s 2007 survey on income and spending, and net annual income flows were calculated as the difference between annual income and expenses. Because the time horizon for the estimate is long, income and spending were projected assuming that the salary projected for 2017 would be maintained over time.
Results
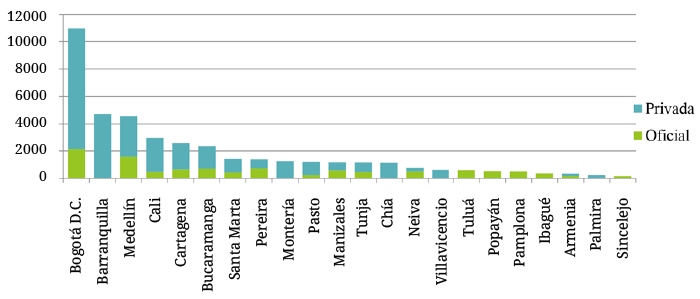
According to the SNIES report, 74 % of all 41, 163 students matriculated to medical programs attend private universities, and 56 % of all the medical students in the country are in Bogotá, Barranquilla, and Medellín. The Colombian municipalities that have only public sector medical schools are Tuluá, Popayán, Pamplona, Ibagué, and Sincelejo, and the municipalities that have only private sector medical schools are Barranquilla, Montería, Chía, Villavicencio, and Palmira (graph 1).
Fifty-three percent of medical students at public universities were concentrated at six of the 18 institutions considered: the Universidad de Antioquia, Universidad Nacional de Colombia, Universidad Tecnológica de Pereira, Universidad Militar Nueva Granada, Universidad Industrial de Santander, and Universidad de Cartagena. Likewise, 40 % of medical students at private universities were concentrated at six institutions out of the 30 considered, if the different campuses of individual universities are grouped together: the Universidad Cooperativa de Colombia, Universidad Libre, Pontificia Universidad Javeriana, Universidad Metropolitana, and Universidad del Rosario.
According to SNIES, the average dropout rate per semester was 3.4 % at the public universities and 6.1 % at the private universities considered. The public universities with the highest dropout rates were the Universidad de Cartagena (9.6 %), Universidad del Tolima (7.5 %), Universidad del Valle (6.1 %), Universidad de Nariño (5.9 %), and Universidad de Pamplona (4.2 %). The private universities with the highest dropout rates were the
Corporación Universitaria Remington (21.2 %), Universidad Santiago de Cali (17.1 %), Fundación Universitaria Navarra (14.1 %), Corporación Universitaria Empresarial Alexander Von Humboldt (12.1 %), and Universidad Cooperativa de Colombia (at its Santa Marta campus) 11.7 %).
Direct Costs
The average total cost of tuition and fees for undergraduate medical education at public universities is US $22, 457. The average total cost of tuition and fees for undergraduate medical education at private universities is US $44, 790. Each of the factors in these totals is detailed below.
Application and Graduation Fees
The weighted average of application fees was US $28.54 at public universities and US $35.01 at private universities. The same values were applied to the counterfactual of non-medical university programs.
Tuition
The weighted average tuition per semester at public universities was US $649 without including State support and US $1806 including State support. The per-semester cost of tuition at private universities was US $3665.
Total tuition for all semesters of the program at public universities, without considering State funding, was US $7932. When State funding was included, total tuition was US $22, 369. At the private universities, total tuition for all semesters of the program was US $44, 790.
Average tuition for the 10 semesters of programs other than medicine was US $5869, US $1831, and US $15, 123 at public universities taking State contributions into account, public universities without considering State contributions, and private universities, respectively.
Graduation Fees
The weighted averages of graduation fees were US $59.82 at public universities and US $191.33 at private universities. The same values were applied to the counterfactual of University programs other than medicine.
Spending Related to University Attendance and Required Equipment
It was calculated that medical students at public universities spend a total of US $14, 613 for the costs of attending university and the purchase of medical equipment during the semesters that make up their programs, and medical students at private universities spend US $18, 063 for these purposes during the semesters that make up their programs. The sources for this data and related calculations are described in more detail below.
The survey was circulated from August 5-30, 2016. Results were obtained from 484 students ranging from their first to their twelfth semester of medical studies at 42 different universities. They included 246 students (51 %) from public universities and 238 students (49 %) from private universities. The greatest number of responses came from the cities of Bogotá, Pereira, Cali, and Pamplona. Adding up all categories of spending per semester, it was found that medical students spend an average of US $1329; more specifically, students at public universities spend US $1187 and students at private universities spend US $1475. Students reported that their largest category of spending (US $526 and US $649, respectively), was for housing, followed by spending for food (US $358 and US $436), transportation (US $180 and US $262), academic books (US $54.89 and US $66.38), photocopies (US $41.13 and US $32.14), biosecurity equipment (US $16.65 and US $16.14), and notebooks and other school supplies (US $10.85 and US $12.99).
It was calculated that students spent a total of US $367 on medical equipment during their undergraduate medical studies.
Indirect Costs
University students in medical programs forgo income of US $17,892 during their six years of study. Students in programs other than medicine forgo an income of US $15, 027 in their five years of study.
Total Cost of Studying Medicine
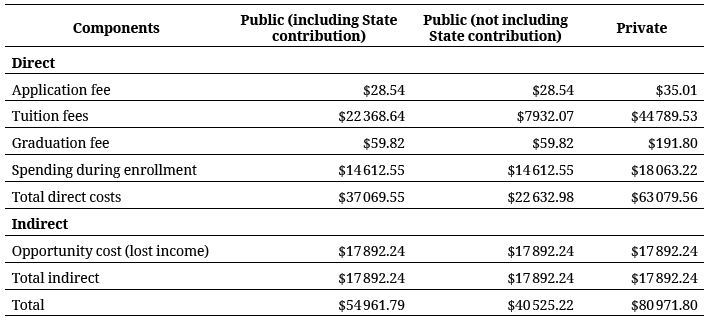
Total direct costs were calculated at US $22, 632 for students at public universities, or US $37, 070 if State contributions are taken into account, and US $63, 080 for students at private universities. Total indirect costs were US $17, 892. Thus, the cost of training a physician in Colombia is US $54, 962 at a public university and US $80, 972 at a private university.
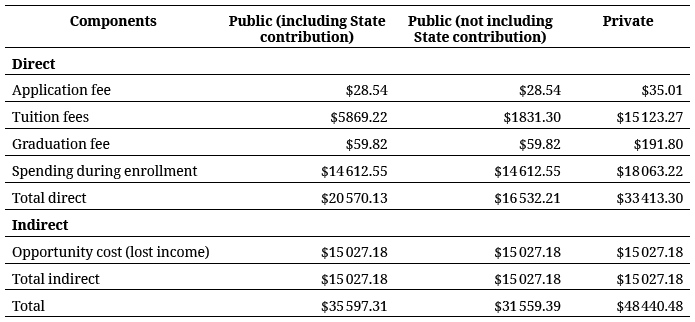
Training a non-medical professional in Colombia, on the other hand, costs US $35,597 at a public university and US $48, 440.at a private university.
Tables 2 and 3 present a summary of the costs entailed in training a physician and a non-medical professional in Colombia, at public and private universities, respectively.
Return on Investment
Table 4 presents calculations on the economic returns from investment in a university undergraduate medical program, and a university non-medical program, for the purpose of providing a baseline scenario (a discount rate of 12 %, constant income, and without considering expenditures) for both public and private universities. Because State contributions to this investment are not assumed directly by the individual, but are returned through taxation and the value of his or her service to society, projections are also made considering exclusively the cost assumed by the individual and his or her family for the professional training received.
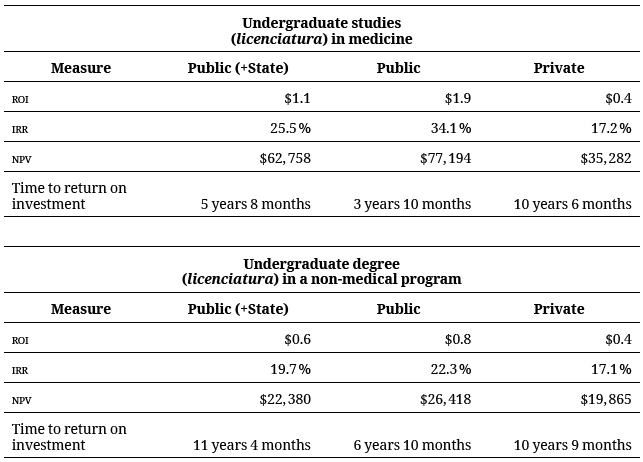
It can be observed that the NPV is positive on a 40-year time horizon subsequent to the completion of the undergraduate program (licenciatura) in medicine. It can also be seen that the NPV is positive for graduates from both public sector and private sector universities, though more so for graduates from public sector universities. This distinction is related to the lesser initial investment for studies at public sector universities under the assumptions made for the purposes of this analysis. The ratio of ROI is positive. Every peso invested in an undergraduate medical program at a public university produces 1.2 pesos while every peso invested in such a program at a private university produces only 0.5, i.e. half a peso. The IRR was estimated at 22.3 % for the licenciatura at public universities and 17.1 % at private universities, greater in both cases then the discount rate applied. As for the time to return on investment, it can be observed that graduates of public universities require 3 years and 10 months to obtain positive benefits while graduates of private universities require 10 years and 6 months to obtain positive benefits. Returns from obtaining an undergraduate degree in a field other than medicine are also favorable, but they are not equal to the benefits obtained by earning an undergraduate degree in medicine. With the exception of the NPV, however, the values obtained after graduating from a private university are very similar in both medical and non-medical fields. This distinction is more significant for graduates from public universities. Despite the high costs associated with studying in an undergraduate medical program, greater benefits accrue from undertaking medical studies due to the higher income of physicians in comparison with practitioners of other professions.
Sensitivity Analysis
A sensitivity analysis was conducted, applying different discount rates (5 % and 7.5 %). The benefit values were higher with both rates and the time required for the return on investment was reduced from that of the baseline scenario. The undergraduate program in medicine produced a greater return than that obtained from any other undergraduate academic program.
In another an analysis of sensitivity, annual 5 % increments to the minimum salary were considered, based on salary increments reported in recent years. It was found that increased income based on minimum salary increments produced greater returns than in the baseline case. Under this scenario, the undergraduate program in medicine continues to produce greater returns compared to other undergraduate academic programs.
In another projection, returns on investment are evaluated in light of monthly spending, taking into consideration average spending and spending for the corresponding income decile. This analytical perspective produced negative returns for both medicine and other undergraduate programs. Results as interpreted from measurements of return on investment can be highly variable depending on the level of spending selected.
Discussion
This is the first Colombian study in which the direct and indirect costs of training a physician and the return on investment over time are estimated. With respect to the economic cost of tuition and fees, private universities receive no State contributions, so the economic burden falls entirely on the student and his or her family.
Although there are few similar cases in the literature on Latin America, researchers in other parts of the world have studied the economic conditions of the student population and the cost of training physicians. One study at the National University of Singapore found that more than 30 % of students took on educational loans, a circumstance that can be attributed in part to the obstacle presented by the high cost of medical education (19). It was estimated that tuition fees alone cost a total of US $87, 459 (US $89, 244 at 2016 constant prices) for the entire program, and US $4470 (US $4561 at 2016 constant prices) annually for other expenses (food, lodging, transportation, public services, medical instruments, and others) (19). Comparing the values found in our study (without considering other calculated costs), we found that the cost of training physicians in Singapore was much higher than in Colombia. In the United States, a 2003 study by Morrison estimated the cost of four years of medical education at public universities (tuition, housing, books, and instruments) to be US $140, 000 (US $149, 717 in 2016 constant prices) and US $225, 000 (US $240, 616 in 2016 constant prices) at private universities (20). This was even higher than in Singapore, whether analyzed as net cost or in relation to per capita Gross domestic product GDP.
In addition, the resources provided by a student for his or her tuition at public universities makes up only a part of the total cost that is assumed for the full training of a physician. In a 2012 study carried out at the University of Sidney, it was found that the annual cost of educating a medical student was US $40, 150 (at 2016 constant prices), most of which (61 %) went to paying the salaries of academic personnel and paying for academic research (21). Students, however, contributed only 17 % of these costs, since the government made significant contributions through its scholarship fund, the Federal Government Commonwealth Grant Scheme, amounting to 36 % of the total, and other university sources contributed an additional 45 %. By comparison, in Colombia the annual cost of tuition is US $3,612.55, of which students contribute US $1297.02, or 34 %.
In 2012, the Organization for Economic Cooperation and Development (OECD) reported an average annual investment per student in tertiary education (university level) of US $9223, or US $9454 at 2016 constant prices (22). These figures are greater than the average annual per-student contribution of the Colombian State to public universities of US $1737, and the difference increases when the current peso to dollar exchange rate is factored in.
According to the OECD report Education at a Glance 2015, university graduates in OECD member countries earned an average 60 % higher income than secondary school graduates (22). This contrasts with the estimated earnings of rural physicians and medical graduates in our study, which can be up to four times higher than the earnings of secondary school graduates. It is notable that the OECD estimate does not distinguish among professionals in different fields, and that university medical programs usually require more academic work and last much longer then professional programs in other fields, which could justify the earnings gap and suggest that this may also be the case in OECD countries, but that the effect was diluted in the report by the averaging process.
In the United States, a 2010 study calculated that return was positive after four years at any discount rate (6, 8, 10 %). In Colombia, however, at least 7-8 and up to 10 years are required, with discount rates of 5, 7.5, and 12 % respectively, to get a positive return on investment (23). The study also showed that annual education costs greater than US $140, 000 would be above the break-even point according to the NPV, and would be characterized as overpriced. This indicates that although tuition fees in the United States are significantly higher than in Colombia, higher doctors’ salaries in the United States allow them to recover their investment more quickly than general practitioners in Colombia.
It can be observed in general terms that the cost of physician training in Colombia is considerably lower than in other countries such as the United States. At the same time, returns on this educational investment are lower than in other parts of the world. If we consider only the local context, however, it can be noted that the returns available to a general medical practitioner in Colombia are greater than those of non-medical professionals, since the latter earn lower salaries.
This research has been limited by the assumptions that were applied, the availability of information related to tuition costs for all public universities, and State contributions to those costs, which vary by discipline. In our analysis, we assumed application and graduation fees in fields other than medicine to be equal to those in medicine. This equivalency, however, would in fact depend on the fee structures at individual universities. Nevertheless, these fees are minor compared to tuition fees, and it is not expected that variations in application and graduation fees would have a significant effect on the results obtained. Assuming that State support for medical programs is similar to support in other fields of study surely underestimates the true cost of physician training in the public sector. Uncertainty is introduced with respect to estimated returns on investment if the spending of graduates is considered, since the measures applied are highly sensitive to graduates’ spending levels. It is also questionable to assume that earnings are constant over time, i.e. without considering physicians’ years of experience.
Likewise, no consideration was given to physicians who continue their studies in a medical specialty, which, on the other hand, was done when the costs of physician training in the United States were estimated (24). Taking this circumstance into consideration would undoubtedly open up possibilities for new pathways of research in Colombia. It would also be worthwhile to analyze regional differences, because different income levels may attract concentrations of general practitioners seeking better-paid employment in areas where their services may not be most required. There is no question that further research should be conducted in this area, because it provides important information that can be used in the development of public policy.
References
1. Adashi EY, Gruppuso PA. Commentary: the unsustainable cost of undergraduate medical education: an overlooked element of U.S. health care reform. Acad Med. 2010;85(5):763-5. doi: 10.1097/ACM.0b013e3181d5cff7
2. Franzini L, Low MD, Proll MA. Using a cost-construction model to assess the cost of educating undergraduate medical students at the University of Texas-Houston Medical School. Acad Med. 1997;72(3):228-37.
3. Gammon E, Franzini L. Revisiting the cost of medical student education: a measure of the experience of UT Medical School-Houston. J Health Care Finance. 2011;37(3):72-86.
4. Rein MF, Randolph WJ, Short JG, Coolidge KG, Coates ML, Carey RM. Defining the cost of educating undergraduate medical students at the University of Virginia. Acad Med. 1997;72(3):218-27.
5. Jones RF, Korn D. On the cost of educating a medical student. Acad Med. 1997;72(3):200-10.
6. Alexander NJ. White. No The high cost of being an (aspiring) medical student. CMAJ. 2008;179(11):1228. doi: 10.1503/cmaj.081284
7. Sistema Nacional de Información de la Educación Superior (SINIES). Indicadores de gestión de las universidades públicas 2012. Avaliable from: http://www.mineducacion.gov.co/sistemasdeinformacion/1735/w3-article-212353.html
8. Rosselli D, Otero A, Heller D, Calderón C, Moreno SPA. La medicina especializada en Colombia: una aproximación diagnóstica. Bogotá: Centro Editorial Javeriano, CEJA; 2000. 224 p.
9. Rosselli D, Otero A, Heller D, Calderón C, Moreno S, Pérez A. Estimación de la oferta de médicos especialistas en Colombia con el método de captura-recaptura. Rev Panam Salud Pública. 2001;9(6):393-8. doi: 10.1590/S1020-498920010006000069
10. Ministerio de Educación Nacional de Colombia. ¿Qué conceptos básicos debe tener presentes? 2016. Avaliable from: http://www.mineducacion.gov.co/1759/w3-article-236683.html
11. Ministerio del Trabajo. Salario mínimo legal en Colombia Banco de la República. 2014 Avaliable from: http://www.banrep.gov.co/es/indice-salarios
12. Sistema Nacional de Información de la Educación Superior (SINIES). Resumen de indicadores de educación superior [internet]. Estadísticas de educación superior. 2015 [citado 2017 feb 14]. Avaliable from: http://www.mineducacion.gov.co/sistemasdeinformacion/1735/w3-article-212350.html
13. Jiménez Boulanger F, Espinoza Gutiérrez CL, Fonseca Retana L. Ingeniería Económica. Primera ed. Editorial Tecnológica de Costa Rica; 2007.
14. Organización para la Cooperación y el Desarrollo Económico (OCDE). Panorama de la educación 2008: Indicadores de la OCDE [internet]. 2008 [citado 2017 feb 14]. Avaliable from: http://www.oecd.org/education/skills-beyond-school/41262207.pdf
15. Observatorio laboral para la educación. Situación laboral de los graduados [internet]. 2014 [citado 2017 feb 14]. Avaliable from: http://www.graduadoscolombia.edu.co/html/1732/w3-article-344801.html
16. Ministerio de Educación Nacional de Colombia. Observatorio laboral para la educación [internet]. 2016 [citado 2017 feb 14]. Avaliable from: http://www.mineducacion.gov.co/sistemasdeinformacion/1735/w3-article-212301.html
17. Ministerio de Salud y Protección Social. Resolución 2358 de 2014: Por la cual se establece el procedimiento para la asignación de las plazas del Servicio Social Obligatorio (SSO), de las profesiones de medicina, odontología, enfermería y bacteriología, en la modalidad de prestación de servicios. (2014 jun 16). Avaliable from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/resolucion-2358-de-2014.pdf
18. Ministerio de Salud y Protección Social. Plazas disponibles para la asignación del Servicio Social Obligatorio del 19 de julio de 2016, según lo reportado por las direcciones territoriales de salud [internet]. 2016 [citado 2017 feb 14]. Avaliable from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/TH/Plazas-Disponibles-20160615.pdf
19. Ng CL, Tambyah PA, Wong CY. Cost of medical education, financial assistance and medical school demographics in Singapore. Singapore Med J. 2009;50(5):462-7.
20. Morrison G. Mortgaging our future--the cost of medical education. N Engl J Med. 2005;352(2):117-9. doi: 10.1056/NEJMp048089
21. Goulston K, Oates K, Shinfield S, Robinson B. Medical student education: what it costs and how it is funded. Intern Med J. 2012;42(10):1149-52. doi: 10.1111/j.1445-5994.2012.02912.x
22. Ministerio de educación industria y deporte. Panorama de la educación. Indicadores de la OCDE [internet]. 2015 [citado 2017 feb 14]. Avaliable from: http://www.mecd.gob.es/dctm/inee/internacional/panorama-de-la-educacion-2015.-informe-espanol.pdf?documentId=0901e72b81ee9fa3
23. Kahn MJ, Nelling EF. Estimating the value of medical education: a net present value approach. Teach Learn Med. 2010;22(3):205-8. doi:10.1080/10401334.2010.488206
24. Ben-Ari R, Robbins RJ, Pindiprolu S, Goldman A, Parsons PE. The costs of training internal medicine residents in the United States. Am J Med. 2014;127(10):1017-23. doi: 10.1016/j.amjmed.2014.06.040
Notes
4 TRANSLATOR’S NOTE Colombian cities and municipalities classify their populations into distinct groups, known as strata, between 1 (the lowest) and 6 (the highest). Each stratum has similar social and economic characteristics. Higher-stratum residents pay more for utilities and public services while lower-stratum residents pay less.
Author notes
* Yaneth Gil-Rojas, PC
** Fabián Hernández, PC
*** Camilo Castañeda-Cardona, MD
**** Pieralessandro Lasalvia, MD
***** Diego Rosselli, MD, MEd, MHPCorresponding author: diego.rosselli@gmail.com
Conflict of interest declaration
This project was financed by the Colegio Médico Colombiano.